![]()











Snowbanks on the Runway
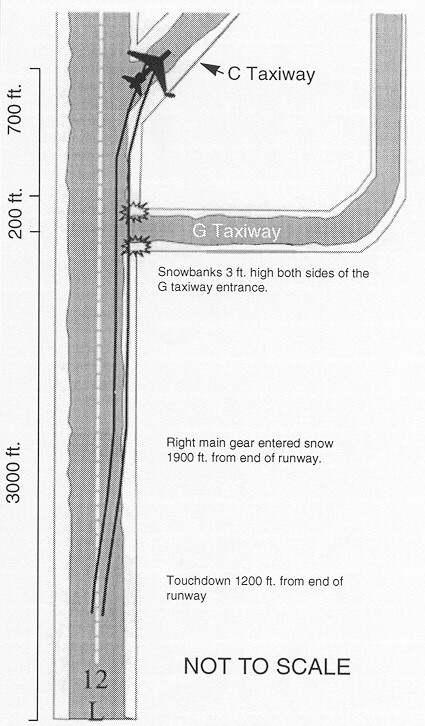
On March 14, 1997, an empty Boeing 727 was returning from Winnipeg, Manitoba, to Hamilton, Ontario. The flight crew conducted an instrument approach to Runway 12L at Hamilton International Airport, with snow-clearing operations interrupted to allow the aircraft to land. The aircraft touched down on the centre line of the icy runway 200 ft. wide and drifted to the right, encountering snow and slush on the uncleared portion of the runway. The aircraft continued to travel in the contaminant along the right side of the runway until the right-hand landing gear struck two three-foot snowbanks lying at 90 degrees to the entrance of G taxiway (see graphic). The right main landing gear failed rearward as a result of the contact with the two snowbanks.
When the right main landing gear failed, the right wing dropped and the wing spar settled down onto the two right main tires. The right wing tip contacted the ground and took out several runway edge lights as the wing tip slid along the ground. The aircraft yawed to the right and came to a stop on C taxiway. The three crew members were uninjured and exited the aircraft via the forward left door, using the emergency rope. The aircraft was substantially damaged.
In its Final Report A97H0003, the Transportation Safety Board of Canada (TSB) determined that the aircraft drifted to the right on the contaminated runway because of stronger than reported crosswinds. The aircraft hit snowbanks left on the runway during snow removal operations, causing the right main landing gear to fail in overload. Other factors contributing to the occurrence were that the flight crew applied an erroneous low wind speed to the landing calculations, and an equipment operator did not notify anyone of the snowbanks on the runway because of a misunderstanding by some ground crew and tower personnel that the uncleared portions of runways are unusable to aircraft.
Among its findings, the TSB determined that the airport anemometer was indicating lower-than-actual wind speeds because of an ice buildup on the anemometer. Although the tower notified the flight crew that the wind speed could be stronger than reported, the crew kept their crosswind calculations based on the reported winds.
Transport Canada (TC) convened a working group to examine the issue of turbo-jet performance with respect to wet and contaminated runway operations. The working group’s final report, which recommends changes to the CARs, is now before the Commercial Air Service Operations committee for review. If the recommended changes are implemented, crews should be better informed to base decisions when operating to or from contaminated runways.
The TSB sent a safety advisory to the Atmospheric Environment Service (AES) on erroneous readings from ice-contaminated anemometers, highlighting the importance of having accurate wind information, especially during adverse weather and slippery runway conditions. AES, in a letter to the TSB, replied that testing has begun of newly developed ice-free anemometers to qualify them for use in Canada in the air navigation system. As there was a misunderstanding among airport workers that the uncleared portion of a runway is unusable by aircraft, a safety advisory on snowbanks on active runways was sent to TC. The Department replied that it is in the process of reviewing the regulations and standards for airports and will incorporate more stringent requirements concerning snow removal and ice control at airports. In addition to an A.I.P. Canada aviation notice called "Winter Operations — Beware of Snowbanks" issued on January 29, 1998, TC issued Aerodrome Safety Information Circular 98-003, "Active Runway Winter Maintenance" on November 9, 1998. The purpose of the circular is to emphasize active runway winter maintenance awareness, and to recommend that airport operators review their snow removal and ice control plan, especially the sections on snow clearing operations and surface condition reporting.
Optical Illusion or Distraction?
On August 10, 1997, a float-equipped Cessna 180, accompanied by an identical Cessna on a fishing trip, crashed on the south slope of the Rivière aux Mélèzes valley in northern Quebec. The pilot and passenger were fatally injured, and the aircraft was destroyed by the post-crash fire. This summary is largely based on Final Report A97Q0168 by the Transportation Safety Board of Canada (TSB).
Both aircraft had taken off around 12:30 p.m. and were flying west over the Rivière aux Mélèzes. The elevation of the valley floor is 300 ft. ASL, and the terrain on both sides of the river rises to at least 1200 ft. ASL. The pilots used a common VHF frequency during the flight. After finding a landing site that appeared suitable, the pilot of the accident aircraft radioed to the other pilot to inspect the site. The latter did a reconnaissance and made a water landing without difficulty. A short time later, the pilot of the accident aircraft initiated a final approach to land at the same spot, but he executed a missed water landing procedure before touching down. He then told the other pilot he was going to examine the landing area more carefully and fly another circuit because he was unsure about the strength of the river current. He climbed above the river to about 450 ft. AGL, then turned 90 degrees left onto the crosswind leg. The aircraft levelled off and proceeded toward the south slope of the valley.
About 30 seconds later, the second pilot saw that the accident aircraft was getting close to the rising terrain and still hadn’t turned parallel to the river and valley wall for the downwind leg. The second pilot suggested he watch out for the mountain. A few seconds later, the aircraft pitched up without changing heading, then made two turns; the first was a right turn at a low bank angle to upwind, and the second was steep and to the left to downwind. The aircraft started to lose altitude and pitched up gradually until it struck some trees, then the ground, in a nose-down attitude. Four or five seconds after the impact, a fire started on the right side of the cabin. Thirty to sixty seconds elapsed between the go-around and the accident.
The accident occurred 100 NM southwest of Kuujjuaq, Quebec, in a partially wooded area approximately one-half mile south of the Rivière aux Mélèzes. The area is somewhat hilly and mainly covered with larch trees of average size. The south side of the valley slopes upward at an angle of about 20 degrees. The aircraft came to rest about 450 ft. above the valley floor. The aircraft cut a swath 50 ft. long through the trees before striking the ground. The impact damage and the nose-down attitude of the wreck are consistent with a loss of control following a stall.
Examination of all recovered components revealed no evidence of pre-impact failure or malfunction, no signs of airframe failure, flight control problems, electrical problems, loss of power, or in-flight fire. No messages were received from the pilot.
According to the TSB report, some situations can severely hinder a pilot's ability to estimate size, distance, speed, or the direction to a slope, or even to identify objects. Pilots can be misled by an optical illusion when approaching rising terrain at right angles. When approaching a ridge, the pilot may tend to maintain a constant angle between the extended cowl and the summit; this causes the pitch attitude of the aircraft to increase while speed decreases. Consequently, aircraft performance decreases and vertical separation with the terrain decreases. The pilot tends to focus on the proximity of the ground, sometimes to the point where flying performance is affected. There is a vivid impression that speed is increasing in relation to the ground, and the pilot may be tempted to reduce speed.
The pilot's decision to fly a left-hand circuit was sound, since he was in the left seat and visibility was better on that side. As the purpose of the reconnaissance was to examine the surface of the water, the pilot had to fly at low level and low speed.
With the aircraft in approximately level flight, it must have closed rapidly with the rising terrain. The pilot did not fly close to the north side of the valley before turning onto the crosswind leg, and as a result, he did not take advantage of all the available airspace in case he needed it. Consequently, not all the space available for the circuit was used to minimize roll attitude in the turns and maximize aircraft performance. The type of circuit selected indicated the pilot intended to do a landing area reconnaissance at low altitude.
Flying in mountainous terrain demands heightened vigilance. Pilots must constantly confirm their impressions with instrument readings. The TSB was unable to determine why the pilot continued flying towards the slope at right angles instead of trying to avoid the ridge until the second pilot warned him. Two hypotheses might explain the pilot's delay in turning onto the downwind leg: he may have been distracted, and/or he may have been misled by optical illusions.
One hypothesis is that the pilot’s attention may have been focussed on planning the water landing or on an untimely event in the cabin. It is possible that, after the go-around, most of his attention was focussed on a continuous examination of the landing area to his left and slightly behind him, and not on flying the circuit. Also, a distraction caused by the passenger feeling the effects of motion sickness or being otherwise indisposed could have produced the same result.
The other hypothesis is that, while flying towards the rising slope, the pilot may have been tricked by an optical illusion, which can be treacherous at low altitude and at near-stall speeds.
After the second pilot called to tell him to watch out for the mountain, the accident aircraft pilot seemed to react, but he did not have much time and his room to manoeuvre may have been reduced to the point where turning around would cause a stall in the turn. The pilot may have assessed the situation and decided to terminate the flight immediately with a forced landing in the best available conditions on the slope of the valley.
The pilot apparently did not have time to cut electrical power and fuel and prepare the cabin for rapid evacuation. Based on the evidence and witness statements, the cause of the accident could not be determined.
Damage to the right wing caused a fuel leak, and, on contact with an ignition source, the fuel ignited and sustained the fire. The witness statements and fire damage suggested that the fire started on the right side of the cabin and the most likely ignition source was electrical; however, the investigation could not identify the source of ignition with certainty.
As a result, the TSB determined that an unknown distraction and/or an optical illusion may have contributed to diverting the pilot's attention from flying the circuit. Although the cause of this accident was not determined, the conditions were conducive to optical illusions associated with flying over rising terrain at low altitude.
The following is an excerpt from the Commercial and Business Aviation Advisory Circular 0141, the purpose of which is to notify pilots and air operators of the potential hazards associated with a low energy balked landing or go-around. Since the circular went only to commercial operators, it was suggested that many private operators could also benefit from the information.
Background — During the aircraft certification process, handling procedures and performance are assessed across a wide range of operating weights, configurations, and flight profiles. The Aircraft Flight Manual defines the boundaries within which the aircraft may be operated safely.
It is a common belief among pilots and many air operators that aircraft are certified to successfully complete a balked landing or go-around from any point during the approach or landing phase. This is not the case.
In brief, an aircraft is not certified to successfully complete a go-around without ground contact once it has entered the low-energy landing regime. The low-energy landing regime is defined as:
- Aircraft flaps and landing gear are in the landing configuration;
- Aircraft is in descent;
- Thrust has stabilized in the idle range;
- Airspeed is decreasing; and
- Aircraft height is 50 ft.* or less above the runway elevation.
* Note: 50 ft. is a representative value. A given aircraft may enter the low-energy landing regime above or below 50 ft. in accordance with approved landing procedures for that type.
Policy — The decision to place an aircraft into the low-energy landing regime is a decision to land. If there is any doubt regarding the probability of a safe landing, a go-around or balked landing must be initiated prior to entry into this regime. An attempt to commence a go-around or balked landing while in the low-energy landing regime is a high-risk, undemonstrated manoeuvre.
In the extreme case where such action is required, pilots should be aware that ground contact is likely and any attempt to commence a climb before the engines have achieved go-around thrust may result in a stall. Turbo-fan engines may require as long as 8 seconds to accelerate from idle to go-around thrust.

On November 19, 1996, a Beechcraft 1900C (B1900) with ten passengers and two pilots was making a straight-in approach at dusk in visual meteorological conditions (VMC) to Runway 13 at Quincy (Illinois, U.S.) Municipal Airport, an uncontrolled airport. A King Air 90 (BE90) with a pilot and passenger-pilot was in takeoff position on Runway 04, which intersected Runway 13. Waiting in the run-up area, second in line for takeoff behind the BE90, was a Piper Cherokee (PA-28). Several seconds before the B1900 touched down on Runway 13, the BE90 began its takeoff run on Runway 04. Despite evasive action by the pilots of both aircraft (a/c), they collided at the intersection of the two runways, killing all aboard. The occupants did not sustain blunt-force injuries that would have impeded their ability to move about or evacuate the a/c, but died from inhaling smoke, soot or other combustion products from the post-accident fire.
The final report of the U.S. National Transportation Safety Board (NTSB) said that "the probable cause of this accident was the failure of the pilots in the [BE90] to effectively monitor the common traffic advisory frequency (CTAF) or to properly scan for traffic, resulting in their commencing a [take-off] roll when the [B1900] was landing on an intersecting runway. Contributing to the accident was the [PA-28] pilot’s interrupted radio transmission, which led to the [B1900] pilots’ misunderstanding of the transmission as an indication from the [BE90] that it would not take off until after the [B1900] had cleared the runway."
The sequence of events — The captain of the B1900 stated on the CTAF that they were about 30 mi. north of the airport and that they would be landing on Runway 13; she also asked that "any traffic in the area please advise." No replies were received to this request. CTAF is a radio frequency designated for use by pilots operating near uncontrolled airports, similar to mandatory frequencies (MF) in Canada. Pilots use this frequency to broadcast their positions or intended flight activities or ground operations.
The passenger-pilot of the BE90 announced that they were taxiing out for takeoff on Runway 04; this was followed by the pilot of the PA-28 announcing that he was "back-taxiing" to Runway 04. The B1900 captain commented to the first officer (F/O), "They’re both using 04. You’re planning on one three still, right?" The F/O replied, "Yeah, unless it doesn’t look good then we’ll just do a downwind for four but ... right now plan one three."
The B1900 captain announced "Quincy traffic, [call sign] is currently 10 mi. to the north of the field. We’ll be inbound to enter on a left base for Runway one three at Quincy, any other traffic please advise." There was no response. Two minutes later, the BE90 crew announced that they were holding short of Runway 04, but would be taking the runway for departure. The report said, "The [B1900] captain...commented "she’s takin’ Runway four right now?" The F/O replied, "Yeah."
The B1900 captain reported on short final for Runway one three and asked "the a/c gonna hold in position on Runway four or you guys gonna take off?" The BE90 passenger-pilot did not respond, but the pilot of the PA-28 did, stating, "[PA-28 call sign] ... holding ... for departure on Runway four..." The B1900 CVR [cockpit voice recorder] then recorded an interruption in the transmission by a mechanical "two hundred" from their ground-proximity warning system. The CVR then recorded the last part of the transmission from the PA-28 as "...on the uh, King Air."
When the PA-28 responded to the question, the B1900 captain believed that she was hearing the King Air crew. The NTSB, however, reports that subtle cues indicated that the transmission did not come from the BE90. Specifically, the speaker gave a different registration number, and the voice was from a male, as opposed to previous transmissions from a female voice in the BE90. ... The PA-28 pilot stated that all the transmissions from both the B1900 and the BE90 were in female voices. "However, because the [B1900] pilots were most likely preoccupied with landing the a/c, and because the speaker said "King Air" and did not say "Cherokee," and the pilots had no reason to expect a response from any a/c other than the BE90, they probably did not notice or focus on those cues."
Although the BE90 had been sitting on Runway 04 for about one minute, the BE90 pilot began the takeoff without making a take-off announcement over the CTAF. Such an announcement would have afforded the B1900 flight crew the opportunity to take evasive action. The PA-28 pilot, who had only 80 hrs of flight time, saw the two airplanes converging, and had the opportunity to alert the B1900 to the situation, which would have been prudent. Despite the 90-degree angle between Runways 04 and 13, the PA-28 pilot stated he did not realize that the runways intersected.
"Because no pilot would take off knowing that another a/c was about to land on an intersecting runway, the occupants of the BE90 must have been unaware at the time they began their [take-off] roll that an a/c was about to land." This lack of awareness could have derived from three sources: failure of the BE90 pilots to monitor the CTAF, mechanical radio problems or the setting of the radio controls on the King Air so the flight crew could transmit but not receive.
"Had the occupants of the BE90 been monitoring the CTAF, they should have heard the four announcements from the B1900 indicating that the a/c was inbound and was planning to land on Runway 13. Because of the extensive fire damage, the settings on the radios at the time of the accident could not be determined."
A time and distance study conducted by the NTSB indicated that the BE90 began its take-off roll about 13 seconds before the B1900 touched down. The occupants of the PA-28 said that the BE90 had been in position on Runway 04 for about one minute before beginning its take-off roll. The PA-28 pilot did not hear a take-off announcement from the BE90 on the CTAF; no take-off announcement from the BE90 was recorded on the B1900 CVR.
The B1900 collided with the BE90 during the landing roll-out at the intersection of Runways 13 and 04. The first people to reach the scene reported that the right side of the B1900 and the BE90 were engulfed in fire. Despite efforts by these people to open the B1900 air-stair door, they were unable to do so. The investigation focussed extensively on the air-stair door, how and why it jammed, its use in an emergency, why nobody could open it from either inside or outside, and its maintenance. "The most likely reason that the air-stair door could not be opened is that the accident caused deformation of the door/frame system and created slack in the door-control cable."
The following are significant excerpts from the NTSB conclusions:
- "The [B1900] crew made appropriate…radio communications and visual monitoring; however, they mistook the [PA-28] pilot's transmission (that he was holding for departure on Runway 04) as a response from the [BE90]..., and therefore mistakenly believed that the [BE90] was not planning to take off until after they had cleared the runway;
- "The failure of the [BE90] pilot to announce over the [CTAF] his intention to take off created a potential for collision between the two [a/c];
- "The occupants of the [BE90] did not hear the transmissions from the [B1900] on the [CTAF]; it is likely that ... the [BE90] occupants did not properly configure the radio switches..., or that they were preoccupied, distracted or inattentive;
- "The occupants of the [BE90] were inattentive to or distracted from their duty to ‘see and avoid’ other traffic;
- "The [PA-28] pilot's transmission in response to the [B1900] was unnecessary and inappropriate and... misled the crew into believing that the [BE90] would continue holding;
- "Because of the [PA-28] pilot’s inexperience, he probably did not realize that a collision between the two a/c was imminent, and therefore he did not broadcast a warning; [and]
- "The occupants of the [B1900] did not escape because the air-stair door could not be opened, and the left overwing exit hatch was not opened."
As a result of the investigation, the NTSB made recommendations to the Federal Aviation Administration on scanning techniques during pilot training and biennial flight reviews, jamming of the B1900 door frame system when it sustains minimal permanent door deformation, methods to ensure compliance with the freedom-from-jamming certification requirements and maintenance oversight.
Editorial note: The many lessons to be drawn from this accident are of interest to all pilots, but, owing to space limitations, we had to focus on the communication and "see-and-avoid" aspects in an uncontrolled environment. Issues such as the jamming of the B1900 air-stair door and the crash response could not be discussed as comprehensively as in the Flight Safety Foundation’s newsletter Accident Prevention, Vol. 55 No. 1, January 1998, from which this article was adapted. Interested readers are encouraged to check it out on the Web at http://flightsafety.org/archives-and-resources/publications/accident-prevention/accident-prevention-1998, or obtain a copy of NTSB Report NTSB/AAR-97-04.














Pilot Resources
Ask ATS
Weather
TSB
Interactive Materials
NOTAMs
Air Safety Institute
ELTs
Aviation Safety Letter
SmartPilot proudly works with.


We would like to acknowledge the financial support of the Government of Canada for this initiative through the Search and Rescue New Initiative Fund (SAR NIF).